Knowledge Transfer / Communication
Each stage of our initiative was linked by knowledge transfer and exchange
(KTE) activities. Through these activities, regional and national stakeholder
groups were engaged in dialogue regarding the goals of the initiative, as well
as the process by which these goals would be achieved. In addition, communications
activities are being undertaken to support future implementation of the project
deliverables.
Methodologies
CEQM maintained stakeholder relationships via the development of a regional
outreach plan using local opinion leaders as knowledge brokers for the project:
- Utilized existing knowledge exchange relationships and also created new
links with knowledge brokering organizations such as the Manitoba Centre
for Health policy which hosted presentations regarding this project.
- Content of dialogue sessions included a focus on primary mental health
care, quality measures as well as future implementation of the project
- Developed project and public websites
- Employed both electronic and print dissemination methods
- Project members, site leads, and identified stakeholders will work collaboratively
to submit publications to academic journals
- Established linkages with other related projects
- Presented in major national research forums regarding primary mental health
care and quality measurement.
Goals
Educate, inform, and share knowledge with stakeholders
regarding primary mental health care and the development of quality measures
through consensus processes
- Create opportunities for dialogue regarding CEQM using KTE best practices
such as KTE networks.
- Ensure support for the work of the project and its implementation at regional
and national levels
- Create general awareness of the project through the creation and maintenance
of a public website
Challenges
The initiative was complex in structure and specialized
to primary mental health care
- Knowledge transfer and exchange was sometimes impeded by the lack of a “common
language” amongst our identified stakeholder groups.
- Budget, human resource and timeline pressures would sometimes inhibit in-depth,
regular communications on a regional basis.
- Managing expectations and priorities of all stakeholder groups was sometimes
hampered by national/regional differences.
- Continued communications with all of the project’s identified audiences
may be required to help with future project implementation; this will require
significant and sustained resources.
Understanding how national & regional Knowledge Transfer & Exchange,
informed and shaped our project activities
Forging Links
CEQM always sought to create its core products, such as quality measures,
based on a distillation of current best practices and activities of primary
health care initiatives across Canada. This was made possible through forging
links with “sister” PHCTF projects, and major national research
institutes (as summarized below) that have been participating in primary health
care and mental health reform activities. It also included links to national
initiatives such as Senator Kirby’s national consultation process regarding
mental health care.
Summary of key linkages:
- The Canadian Institute for Health Information (CIHI),
- The Canadian Health Services Research Foundation (CHSRF) ,
- The Saskatchewan Health Quality Council
- The Centre for Addiction and Mental Health
- The Canadian Collaborative Mental Health Initiative (CCMHI),
- The Winnipeg Regional Health Authority
- The Manitoba Centre for Health Policy.
- UBC Centre for Health Services and Policy Research (CHSPR) Primary Health
Care Logic Model project.
Maintaining Dialogue and Feedback loops
Our use of KTE and consensus building between diverse groups of stakeholders
helped maintain a dialogue over a three year span which in turn helped improve
the project. From this dialogue we also learned how the project could be implemented
locally and we were able to assume a “knowledge broker” role, sharing
knowledge about projects in primary health care from coast to coast. These
dissemination activities should increase uptake of the final results of the
initiative across Canada. If this knowledge exchange process continues to be
supported, it should allow for an enhanced degree of inter-regional collaboration
on future health system reform.
Consumer/consumer advocates included in our research and dissemination
Our dissemination activities made a concerted effort to include consumer/people
living with mental illness/ user perspectives. We had a high rate of participation
from these stakeholders in our surveys and focus groups. Amongst these groups,
our emphasis on primary mental health care was seen as both unique and very
much needed. We heard that stakeholders appreciated the opportunity to be involved
in the shape of the research and were interested in seeing our findings used.
A focus on regional and national knowledge exchanges
At the regional level, KTE sessions occurred in a variety of formats such
as:
- contributing to the agenda of existing regional organization/association
meetings;
- informal networking at relevant meetings, conferences or events;
- Dialogue with individuals or small groups at regionally-based academic
centres.
- On-line information sessions using web based and telephone conferences.
National Knowledge Transfer & Exchange
At the National level, an overview of the project and results from the first
survey were presented in a series of KTE events across Canada with multi-stakeholder
participants. These sessions provided an overview of the project, opportunities
for discussion and dialogue (including capturing of stakeholder feedback) and
distribution of communication collateral (project brochures).
Capitalizing upon KTE activities: A KTE network
We sought a commitment from individuals in national and regional KTE forums
regarding participation in a national PMHC measurement KTE Network. To date,
approximately 270 individuals with representation from every province and territory
have agreed to participate. This potential network would be a first step in
fostering continued pan-Canadian collaboration regarding implementation of
PMHC quality measures.
Summary of National KTE events:
| September 24, 2004 |
|
The Centre for Addictions and Mental Health in Toronto, ON |
| September 24, 2004 |
|
Ontario Ministry of Health, ON |
| November 22, 2004 |
|
The Federal/Provincial/Territorial Mental Health Advisory
Network in Toronto, ON |
| March 17, 2005 |
|
Health Quality Council of Saskatchewan in Saskatoon, SK |
| March 23-24, 2005 |
|
Key Regional Stakeholders in Quebec City and Montreal, PQ |
| March 23-24, 2005 |
|
Public Health Agency of Canada (PHAC) Mental Health Surveillance
Workshops in Ottawa, ON |
| April 6-7, 2005 |
|
Health Canada presentations, including PHAC, PHCTF, and FNIHB
in Ottawa, ON |
| April 11-12, 2005 |
|
The Canadian Health Service Research Foundation (CHSRF) National
Workshop on Primary Health Care in Vancouver, BC |
| May 18-19, 2005 |
|
Canadian Institute for Health Information (CIHI) Conference
on Primary Health Care Indicators in Toronto, ON |
| June 10-13, 2005 |
|
6th Annual Shared Care Conference in Ottawa, ON |
| June 15, 2005 |
|
Manitoba Centre for Health Policy in Winnipeg, MN |
| September 18, 2005 |
|
Presentation of the project’s Stage 2 best practices
at the International Conferences on the Scientific Basis of Health Services
(ICSBHS) in Montreal, PQ |
| December 7, 2005 |
|
National KTE Event, Toronto, ON |
| February 2006 |
|
Research work on facilitators and barriers to implementing
quality measurement in primary mental health care presented at the Primary
Care Conference held in Calgary, AB. |
| May 1, 2006 |
|
Preliminary Final Results presented at Shared Care Conference,
Calgary, AB. |
| September 1, 2006 |
|
KTE events, Toronto ON and other ON sites, including Sudbury
and Peterbourough |
| September 13, 2006 |
|
Québec KTE event with 43 stakeholders |
| September 2006 |
|
Final Results and launch of Quality Measures Database presented
at the Primary Health Care Symposium, CHSRF, Vancouver, BC. |
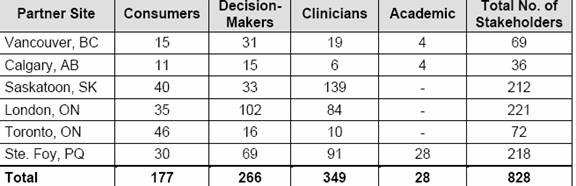
Extent of regional and national KTE participation
From April 2004 to March 2005, a total of 828 stakeholders participated in
dialogue about the initiative. The table below outlines the total number of
stakeholders targeted per participating region during 2004/05.
Team Lead
Renée Sarojini Saklikar
National Knowledge Transfer Advisor
CARMHA
Centre for Applied Research in Mental Health & Addiction
Faculty of Health Sciences, Simon Fraser University
renees@interchange.ubc.ca
Other team members
Carol Adair
Denise Aubé
Donald Addington
Ellen Anderson
Clay Barber
June Bergman
Ulrieke Birner
Monique Carriere
John Conway
Alex Craciunescu
|
Martha Donnelley
Jennifer Hermann
David Haslam
Terry Isomura
Tania Kyle
Alain Lesage
Elizabeth Lin
Eric MacNaughton
Leann Meronek
Mike Pennock
|
Léo-Roch Poirier
Radha Puri
Mélanie St-Onge
Elizabeth Tovey
Ellisa Wee
Roger Wheeler
Natasha Zaslavska |
v5 Sep 27, 2006
Copyright © 2006 CEQM and CARMHA • info ceqm-acmq.com
ceqm-acmq.com
The views expressed herein do not necessarily represent the
official policies of Health Canada
